
Military Spouse Advocacy
Breathing life into clinicians that serve
Leveraging our best assets to solve the military mental health crisis.
The War Department must fully utilize, immediately and effectively, the largest and potentially the finest single source of labor available today- the vast reserve of woman power.
Henry L. Stimson
Secretary of War, 1943
Advocate, Military Spouse Clinician, and CEO of Lifegiver
Military spouse advocacy does not have to be about female employment. But there is a lot we can learn from how World War 2 united the country by employing those back at home and giving them a part to play. It is about leveraging the strengths of the community we already have at our fingertips to create a stronger force- a healthier force that will be able to reintegrate back into society and be our future nation’s leaders.
Corie Weathers, LPC, NCC
Advocate, Military Spouse Clinician, and CEO of Lifegiver

Lessons learned from WWII
Active duty military spouses make up nearly 1 million of today’s American population1, millions more are married to a veteran. While not all spouses are women, 92% are2 and they are talented, gifted, and equally loyal to their country.
World War II got something right. It was out of necessity that leveraged close to 6 million women into the workforce to support war efforts and fill in the vacancy left behind by the draft. The result was the integration of those who were sent with those who sent them.
Lessons learned from Vietnam
Following Vietnam, we realized more than ever that our servicemembers and their families not only need the support of the country they served, but the mental health care to be able to reintegrate back into society. With a current suicide rate of 22 veterans a day (including some of our most recent young veterans) and military spouse suicide on the rise, having mental health providers that are trained, passionate, and culturally competent in the challenges and strengths of military life is crucial.
What if we had everything we needed to address the mental health needs in military families?
Military spouses can be that answer...

Military spouse behavioral health clinicians are already culturally competent, experienced, loyal, and ready to serve.
Telehealth: A modern approach to mental health Care
OUR NEED: Culturally competent clinicians that can provide mental health care face-to-face and remotely to those in rural locations or are appropriate for online telemental health.
We know that military families and veterans prefer culturally competent clinicians that not only understand them, but are passionate to see them whole.3 In addition, they want to use their benefits in order to financially afford the mental health care they need. This is most often through Veteran Affairs (VA) and Tricare. This means they need clinicians that preferably have lived the lifestyle, contracted with their benefits, and quickly and conveniently located.
OUR ANSWER: Utilize military spouse mental health clinicians as culturally competent assets to treat the mental health needs of military families through telemental health.
Military spouse clinicians are:
- Already competent in the lifestyle
- Licensed providers
- Wanting to serve their country and military community
- Becoming more creative in their use of telehealth as a solution to their career portability & the needs of families they serve
Are you a military spouse mental health clinician or student?
So what's the problem?
my story as a military spouse clinician
Current issues
- Military families struggle to locate culturally competent mental health clinicians that also offer services convenient to the lifestyle when using their Tricare benefits.
- Tricare directories are out-of-date and are not currently set up to feature providers that provide telemental health services state-wide, only brick and mortar locations.
- Further, military spouse providers are discouraged with application/credentialing, address change timelines extending 9 months- year rather than the quoted 90 days. For those relocating, fewer practices are stalling or not able to open.
- Military spouse behavioral health clinicians have discovered telemental health as a creative, remote-work solution to licensure portability now that Tricare covers telemental health. Most counseling state boards (LCSW, LPC, LMFT, etc) approve of telemental health services to citizens in that state regardless of the clinician’s location. However, the Tricare application/claim system is stuck in a “brick and mortar” mentality making it difficult for telemental health providers to enroll without a physical address.
- Providers are ending In-network contracts due to reimbursements rates to opt for higher reimbursement rates as an Out of Network provider resulting in fewer searchable providers in the Tricare database.
What DHA/TRICARE Contracting can do:
Encourage Humana/HealthNet to:
- Expedite the application and credentialing process for military spouse providers with a checkbox on applications AND an internal standard operating procedure for expedition.
- Encourage telehealth-friendly provider applications for those without a physical location. Contracts and credentialing can be state-based with an internal provider mailing addresses. Military spouses will be able to relocate and not have to update practice locations or directory listing.
- Modernize the TRICARE directories to search beyond zip codes by including In AND Out-of- Network providers AND telehealth providers that serve state-wide based on their license.
- Enforce consistency regarding telemedicine rules between DHA Tricare Policy on Telemedicine (Chapter 7 2.2.3.1) [4] and Humana and HealthNet. (See HealthNet’s website). [5]
What can DOD do?
- Encourage state boards to continue to apply laws/rules based on where the CLIENT is located rather than where the provider is located.
- Ask state boards for a 90 day maximum turnaround for expedited military spouse applications, temporary licenses, etc.
- Encourage state boards to not require military spouses to meet state standards while on a temporary license unless it is their first license or they plan to hold a license there indefinitely.
- Advocate for better funding for Tricare reimbursement rates to retain high quality providers (Congress or Humana/HealthNet contracts with providers).
- Open up Federal Behavioral Health Jobs to Licensed Professional Counselors (LPCs)
- Hire more military spouses in Military Family Life Consultant (MFLC) and Military One Source (MOS) mental health positions.
- Market military-wide that they, themselves, can be a partial answer to spouse employment and mental health care for military families by using a hiring campaign for Tricare, and DoD Federal mental health positions.
Everyone Wins!!
- Military spouse clinicians can maintain fewer licenses by continuously serving clients in a state they are licensed in, regardless of relocation.
- Fewer licenses results in lower reimbursement costs for DOD branches.
- Military families have convenient access to a wider network of culturally competent clinicians that can accommodate around military lifestyle challenges all while using their benefits.
- Department of Defense makes progress in military spouse employment and licensure portability by messaging that Tricare will hire more military spouse providers.
- Outgoing health costs are reduced by embracing culturally competent providers that can make progress with fewer sessions.
- States maintain their sovereignty to regulate licenses and protect the public (client).
- Department of Health Agency improves reputation with providers and beneficiaries by increasing provider network, modernizing access to care, and marketing their part in improving spouse employment and licensure portability initiatives.
- State boards are beginning to regulate telemental health ethics with CEU requirements, laws, regulations, and rules for working across state lines.
QUICK FACTS!
Military spouse clinicians are practicing all over the globe with many that are in school, finishing degrees and eager to serve.
Lots of research has been shown in the benefit and effectiveness of culturally competent, military connected clinicians. Click here for more.
” Anecdotal evidence suggests that when servicemembers or veterans seek behavioral healthcare services, the clinician undergoes an initial litmus test of trust that includes the question, “With all respect, are you a veteran?” or “Did you serve?” Failure to earn the servicemember or veteran’s trust, especially during the initial meetings, increases the likelihood that the therapeutic alliance will erode. As such, it becomes imperative for clinicians to develop military cultural competence, particularly if they are not military-connected. ” Click here to read more
” The VA MISSION Act, among other things, removes all geographic and licensing barriers to VA telehealth, thereby allowing veterans to access VA telehealth services in their communities from any location in the United States, U.S. territories, District of Columbia, and Commonwealth of Puerto Rico.” Click here to read more
“Telemental health care can provide effective and adaptable solutions to the care of mental illnesses universally. While being comparable to in-person services, telemental health care is particularly advantageous and inexpensive through the use of current technologies and adaptable designs, especially in isolated communities.” Click here to read more
Get involved...
What can YOU DO?
advocacy
ad·vo·ca·cy| \ ˈad-və-kə-sē
: the action of advocating, pleading for, or supporting a cause or proposal
Are you a military spouse behavioral health clinician? Join the hundreds who have already shared their story and struggle to build their career by taking the survey.
We believe the Rosie Riveters of World War 2 launched one of the most patriotic times in our nation’s history as well as launched a path for female employment that changes the course of history. It is time to see that happen again, for our military, our military spouses, and our country.
We want to record your story. Whether you were a riveter, a nurse, or did any other job that supported the military or service members. Please reach out to us by telling us a little bit about yourself and we will be in touch on how we can help you share your story.
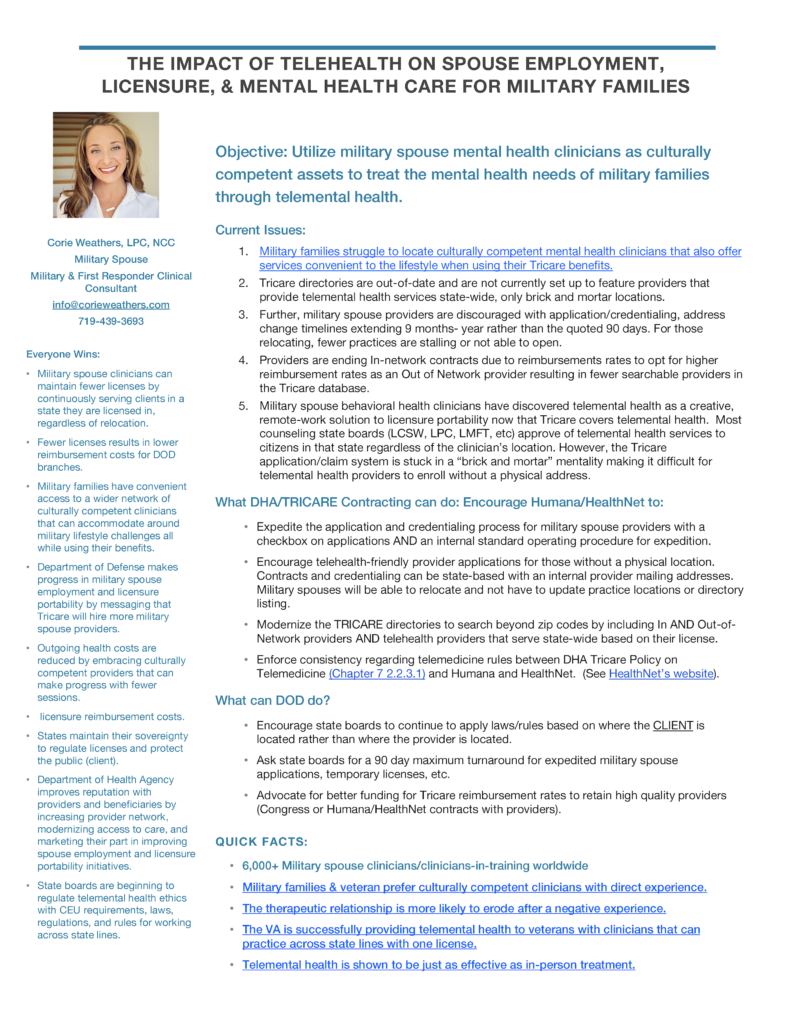 Everything you need to be informed and advocate- all on one sheet of paper. Take this one sheet to your Congressmen, your professional state boards, Governors, the DoD, and those within the Department of Health Agency/TRICARE.
Everything you need to be informed and advocate- all on one sheet of paper. Take this one sheet to your Congressmen, your professional state boards, Governors, the DoD, and those within the Department of Health Agency/TRICARE.
Use the form below to:
- Share your military spouse clinician experience.
- Share how having a culturally competent clinician made a difference for you as a military family or veteran.
- Share interest you have for getting involved.
- Share research that is connected to this cause.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References:
1. (2019). Dhs.gov. Retrieved 22 January 2019, from https://www.dhs.gov/sites/default/files/publications/First_Responder_Market_Overview_Synopsis_2017_508C.pdf.
2. Luby, Christi Ann. “Health Assessment for Loved Ones: Development and Validation of a new instrument to measure well-being in Military Spouses.” PhD Diss., University of Texas, El Paso, 2015.
3. https://militaryfamilyadvisorynetwork.org/wp-content/dl/MFAN-2017-Survey-Report.pdf
4. https://manuals.health.mil/pages/DisplayManualPdfFile/TP08/214/AsOf/TP08/c7s22_1.pdf
5. https://www.tricare-west.com/content/hnfs/home/tw/prov/benefits/benefits_a_to_z/telemedicine_services/telemedicine_details.html
Additional references used:
Telehealth effectiveness: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5723163/
VA Telehealth: https://fas.org/sgp/crs/misc/R45834.pdf
Service Members Prefer a Psychotherapist Who is a Veteran: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6034519/